Neck Safety and Yoga Inversions

Turning the World Safely Upside Down — The Safe Practice of Headstand and Shoulderstand Yoga Poses
Yoga inversions can be a joyful, empowering, perspective-altering experience. They require us to do things with our body that we might not have experienced since childhood. What makes yoga inversions so exciting is the fact we are using our arms and heads in ways we do not normally do. We can also make them high risk, leaving us susceptible to injury. Our necks, in particular, can bear the brunt of injuries in certain inversions.
To understand how to practice yoga inversions safely, let’s first discuss the anatomy of the neck.
Free Range
The neck, or cervical spine, is formed by seven vertebrae that stack on top of each other. The vertebrae form joints with the one above and below, and move by gliding on the joints. The neck has a forward curve known as lordosis. During development, the curve of the neck is formed when we started to lift our heads as infants.
The vertebrae are separated by a disc, which acts as a shock absorber and a pivot point for motion. The exception to this is there is no disc between the first and second vertebrae, which are shaped completely different than the other vertebrae of the spine. The second vertebra-also known as the axis vertebra-has a peg-like protrusion that fits into a hole in the first vertebra, also known as the atlas vertebra.
The cervical spine has a vast range of motion capable of rotation, flexion, extension, and side bending. It has the most motion of all the sections of the spine. This mobility means that stability is sacrificed. As the vertebrae move in relation to each other (gliding on the joints), the discs also move. As the cervical spine flexes forward, the discs move backward, and as the spine moves backward in extension the disc moves forward. The disc is full of a jelly like substance known as the nucleus pulposis, and if the outer fibers of the disc tear, the internal substance can be squished out resulting in what’s known as a disc herniation.
Top as Bottom
When we use our head as our foundation, instead of our feet, we need to recruit stability for an unstable surface. The architecture of our head and neck is such that it is made to float and move, not to bear weight. We need to support our neck and head when we go into poses like Sirsasana, or headstand.
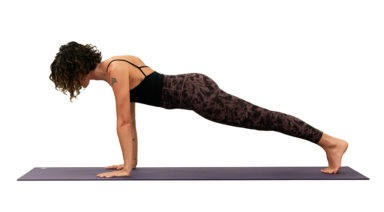
Headstand can help us change our perspective, conquer the fear of inverting, and traditionally is thought to stimulate the pineal and pituitary glands, as well as tone the abdominal organs. There are many variations of headstand (tripod with head and palms on the floor; supported with head and forearms on the floor; and variations of head on the floor with finger tips out and arms extended).
The safest version of headstand is Salamba Sirsasana or supported headstand against a wall. Using the forearms on the mat allows us to recruit the strong muscles of the shoulder girdle and to create space for the neck. It also allows us to distribute our weight between the head and forearms.
Using a wall helps us to avoid awkwardly falling out of the posture. The most common way to injure our discs is when our neck is forced into flexion. This causes the disc to move backward, and if the fibers of the disc tear, the nucleus pulposis center can herniate out, causing irritation to the nearby nerves that exit the spine. These nerves supply the muscles and skin of the arms and hands, and, if injured, can result in months of painful recovery. Unsupported headstand, unfortunately, leaves us vulnerable to this type of injury.
Headstand is an advanced posture and should only be practiced under the supervision of an experienced teacher. Individuals with high blood pressure or ocular disorders should consult a health care practitioner familiar with yoga before proceeding.
Not a Neck Stand
Another common inversion is Sarvangasana or shoulder stand. Shoulderstand can be a great chest opener, a way to relieve swelling in the legs and is traditionally credited with stimulating the thyroid gland and abdominal organs.
Shoulderstand requires us to place the neck into a deep flexion. It is important that we support the cervical spine by allowing weight to rest on the fleshy part of our upper shoulders and back. We can improve this by rolling our shoulders under slightly to begin the pose, so that we are open across the collar bones and help maintain the lordotic curve of the neck.
To take some of the weight off of the neck and upper shoulders, we can practice Ardha Sarvangasana or half shoulderstand. In this version, we do not bring the feet all the way up to vertical, but allow the weight of the body to be well supported by the hands on the lower spine with the body and legs at approximately a 45 degree angle. It is important never to move the head around in the pose to avoid awkwardly weighting the neck.
Shoulderstand is an advanced posture and should only be practiced under the supervision of an experienced teacher. Like headstand, individuals with high blood pressure or ocular disorders should consult a health care practitioner familiar with yoga before proceeding.
The Joy of Limitation
Once we understand the anatomy and mechanics of our bodies, we are better able to practice yoga with respect for our limitations. Knowing what we are capable of and what our potential weaknesses are allows us to challenge ourselves in other ways and opens doors in our yoga practice we may never have thought to open. Embrace the many variations of yoga inversions and enjoy the view from down there.
About the Author

3 Exercises to Strengthen Your Hips and Balance Your Body

In yoga we often speak of tight hips, needing to open the hips, balancing the opening of our hips from side to side (etc), but there is more to a balanced body than open hips. We also need stability and support from our hips. This is important not only in yoga but also in day-to-day activities like simply walking. It is especially important if you are an athlete and need to perform on one leg.
A Look Inside the Hip Our hip musculature is made up of many muscles, large and small. For stability, we need the muscles of the side of the hip to be active and engaged. If you place your hands on the sides of your bony pelvis below your waist, you can imagine a tear-drop-shaped area below the ridge of your pelvis. The front part of the tear is the Tensor Fasciae Latae or TFL which connects with your IT band to join at the knee. At the back part of the teardrop are the Gluteus Medius and Minimus, which lie underneath your big Gluteus Maximus.
These muscles are what support and keep you steady in balance poses or when you transfer weight from one leg to the next as you walk or run. For many of us, these muscles are fast asleep, so we recruit our hip flexors at the front or our glutes and our hamstrings at the back to do a job they were not designed to do. Over time this can lead to low back pain and sacroiliac joint pain. Forcing our body to compensate will lead to problems over time. A look outside the hip Tree pose can be a simple test to see if we are accessing our side/lateral hip stabilizers.
Stand in front of the mirror and take a medium-size tree pose with your foot resting on the shin (even if you can go higher). Place your hands on your bony pelvis again and see if they are level from side to side. If not, press the shin into the foot and the foot back into the leg so that the standing hip drops to make the hips level. If this is too difficult to achieve, keep your foot off the ground but come out of tree pose so that your knee is facing forward, raised to hip level with the knee bent.
Try to level the hips again here by firmly rooting into the ground with the standing leg. My Three Favorite Lateral Hip Exercises Most of us can benefit from a little extra love and attention to the side of our hips. Try these exercises to wake up your hips and begin to stand taller on one leg
1. Kick the Ball Standing: Lift one foot off the ground. Keep your leg straight and send your heel forward, toes pointing out as if you were passing a soccer ball in slow motion. Reverse this motion by turning your toes in and sending your leg behind you. Flow forward and back, heel in and out, in a short arc. Don’t forget about your standing leg: root into the earth and don’t let the hip hitch out to the side. Repeat this motion ten times and then switch sides.
2. Clam Shell: Lie on your side with either your arm or a foam block supporting your head. Bend both hips to 90 degrees with knees bent, feet touching, stacked on top of each other. Slowly lift your top knee up towards the sky while keeping your feet together (as if you were a clamshell opening). Keep your hips stacked and avoid rotating with the pelvis. Lower, repeat times, and switch sides.
3. Bicycle: Lie on your side with both legs straight. Flex your feet, as if standing, and stack them on top of each other. Lift your top leg so that feet are hip-width apart. Keep this distance as you flow through this sequence: a) knee bent move forward to the hip at 90 degrees, b) straighten at the knee, c) float straight leg back to start. This should look like you are slowly pedaling a bike. Keep the hips stacked and stable. Strengthening our lateral hips will not only improve our yoga practice, but will also balance our body and prevent injury so that we continue to walk, vinyasa, and run for years to come.