Yoga and Anterior Pelvic Tilt

The anterior pelvic tilt is a hot topic in yoga and in manual medicine. Some people are overly concerned about the fact that their pelvis is tilting anteriorly without even understanding what it means. Let’s simplify the issues behind this increasingly common postural variation and learn how it can affect other parts of our body.
A normal pelvic angle is 30°; this means that our posterior superior iliac spines (the dimples above our bottoms) are slightly higher than our anterior superior iliac spines (the bones that stick out at the front of our pelvis). This angle can vary a few degrees either anteriorly or posteriorly due to our genetic makeup and even temporarily due to tight and/or weak muscles. An anterior pelvic angle of 40° is considered excessive and will produce a lower back (lumbar spine) curve that is also extreme. Our lumbar spine should have an anterior curve which is known as a lordosis; however, when this curve is excessive it is known as a hyperlordosis, which is not ideal. Cases of increased pelvic angles and lumbar hyperlordoses are very prevalent in today’s society.
Causes of increased lumbar lordosis include:
- Postural deformity
- Lax muscles, especially the abdominal muscles in combination with tight muscles, especially hip flexors or lumbar extensors
- A heavy abdomen, resulting from excess weight or pregnancy
- Compensatory mechanisms that result from another deformity, such as an increased curve in the thoracic spine (mid-back)
- Hip flexion contracture
- Spondylolisthesis (displacement of the vertebra above with relation to the vertebra below)
- Congenital problems, such as bilateral congenital dislocation of the hip
- Fashion (e.g., wearing high-heeled shoes)
Magee, J. David. Orthopedic Physical Assessment: Fourth Edition. Saunders. Toronto. 2002.
Cause number two from the list above is the reason that affects most. The majority of the population sits for at least eight hours a day while hunched over a desk at work; this can lead to a generic condition known as lower cross syndrome. This disorder consists of the following muscular issues: Weak or inhibited gluteal muscles and abdominals & Tight and shortened hip flexors and lumbar extensors
To better visualize this, observe the illustration that demonstrates lower cross syndrome. Take note of how the two weak/inhibited muscles create one line of the cross and the two tight/shortened muscles create the other line to complete the shape of a cross, hence lower cross syndrome.
When our hip flexors are tight, specifically our psoas, our pelvis rotates forward by the psoas pulling down on the lumbar spine from its attachment sites; this increases our lumbar lordosis and subsequently shortens our lumbar extensor muscles. This is most often seen in combination with weak abdominal and gluteal muscles.
Now that the reasons for this postural condition have been noted, the way to correct it is clear: reverse the causes. However, the distinction between inhibited muscles and weak muscles must be made first before rehabilitation can effectively begin. Inhibited muscles require the re-establishment of correct muscle firing patterns, while weak muscles need to be strengthened. Some individuals have weak muscles that are not inhibited; some have the reverse, and some have both issues to correct. Tight/shortened muscles require lengthening; sometimes stretching is sufficient and sometimes alternative soft tissue treatments such as Active Release Technique® and Graston Technique® are required to decrease scar tissue and increase the range of motion of the particular muscle.
If you are concerned that you may have lower cross syndrome, or simply a pelvic tilt, paying a visit to your manual health care practitioner (sports focused chiropractor, sports physician) will be well worth the time and money. They will be able to diagnose any underlying issues related to this condition and create an appropriate rehabilitation programs specific to the weaknesses and inhibitions they find upon physical examination. They will also be able to reduce scar tissue that may be contributing to your pelvic tilt (anterior or posterior).
Education is the ticket to eliminating these sorts of conditions from society. If we understand how to mitigate the risks for such generic conditions, we will all be much healthier individuals. Here is to learning more about our bodies!
Learn More about Dr. Carla Cupido.
About the Author

Yoga Anatomy: Reducing Shoulder Impingement

![]()
![]()
Our wonderful shoulders are the most mobile joints in the body and, for anyone who has done any amount of Hatha Yoga flow, we can appreciate how much the shoulders are engaged and challenged in our practices. Given how frequently we load and stress the shoulders in yoga, it is ideal to move the shoulders with intelligence, mindfulness, and attentive care. One aspect of mindful movement and engagement is reducing the onset of shoulder impingement.
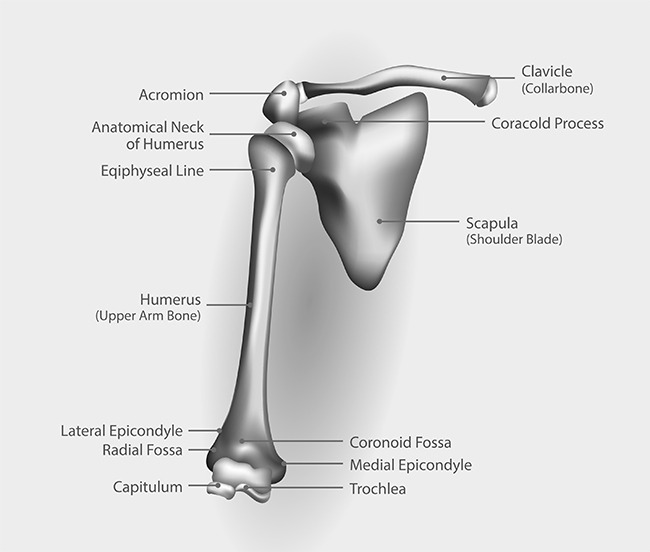
Our shoulder joints are made from a ‘ball and socket’ design. The upper arm bone (humerus) has defined structures at its proximal end (closest point to the center of the body). At the proximal end of the shaft, we see that the humerus has boney processes (called tubercles where tendons attach). Moving towards the shoulder joint, the humerus has a neck that transitions into a ‘head’ or the ball portion of the joint. The humeral head inserts into the socket (glenoid fossa or cavity) forming this highly moveable joint. The socket is part of the shoulder blade (scapula bone). There is another part of the shoulder blade with a boney projection called the acromion process which is positioned above the humerus. You call feel the acromion process on yourself by taking one hand over and to the back of the shoulder blade. Run your fingers along the shoulder blade to find a horizontal line of bone – this the spine of the scapula. Run your fingers all the way to the end into your shoulder – where this ends is your acromion process.
Between the acromion process and the tubercle region of the humerus is the ‘subacromial space.’ This is where our attention goes regarding shoulder impingement considerations. Deep above the spine of the scapula runs one of your rotator cuff muscles (supraspinatus muscle), which has its tendon traveling through the subacromial space and attaching onto the greater tubercle of the humerus. To offer some protection to this tendon, there is a small sac of fluid (bursa sac) between the tendon and the acromion process.
When we stand in Mountain pose (arms relaxed), there is ample space in the subacromial space for the supraspinatus tendon and the bursa sac. When we lift our upper arm bone outwards (abduction) or towards certain angles of significant forward movement (flexion), the humerus closes into the subacromial space. For some people, due to bone structure and reduced subacromial space, they are more prone to having the tendon and/or bursa sac being compressed and stressed (aka shoulder impingement). With frequent compression, the tendon and/or bursa sac may develop conditions of inflammation. As with any acute or chronic development of shoulder impingement conditions, you will want to consult a qualified health professional for proper assessment and therapeutic treatment.